
At the oncologist appointment in January I got my MRI results and later the accompanying report. The oncologist said the PSA indicated the cancer was still active - it had gone from 5.5 in November, 2.6 in December to 9.1 in January and 8.3 in February. His recommendation was to start hormone treatment immediately for three months then have a month of radiation; the concern, as always, is that waiting can lead to cancer metastasising.

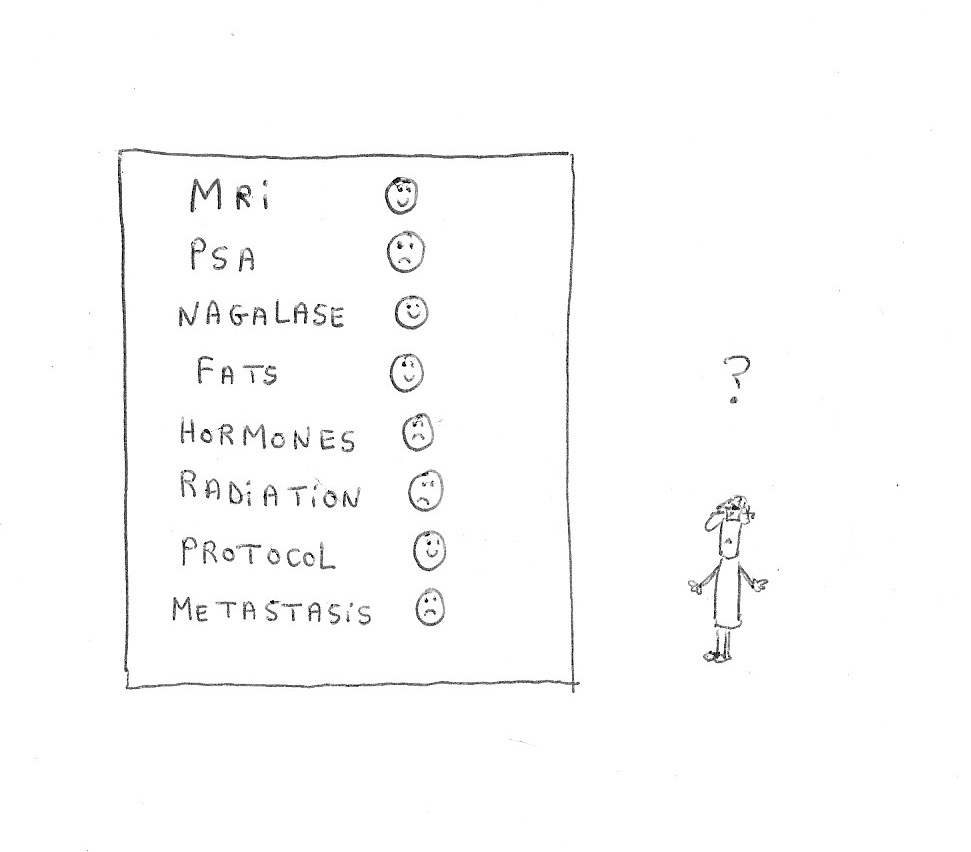
It is also not done without fear and concerns; am I really making the best choice? Here are some of the things I have considered in deciding to delay:
1. MRI says 'no change'
The report, which the oncologist was fairly dismissive of, says ’no change’ compared to my previous MRI eighteen months earlier. In fact when I got the report a couple of weeks later it stated that the prostate is smaller ie 40ml where previously it was 56ml (although the ultrasound showed 40ml first time around). There is also only one unchanged focus in the left lobe, whereas before others were seen plus no pelvic adenopathy (distortion of lymph nodes); there is also no regional lymph nodes metastasis compared with 9mm diameter pelvic node before. The caveat is that there was some blurring in the scan which interfered slightly with definition. So my ‘invasive’ and ‘aggressive’ cancer is probably smaller and certainly not bigger. The treatment in Germany, change of diet, supplement regime and all the other things I am doing must be working to some extent.
Interestingly when my cancer was first diagnosed I was given a T2a by the radiologist but then it was corrected to 'definiately' a T3a. Now the rating in January was given a T2b/T3a. It is clear that it is difficult to read accurately these tests - that's just the nature of the beast! I seem to be on the borderline between a serious and less serious cancer?
 |
| MRI Jan 2091 |
Interestingly when my cancer was first diagnosed I was given a T2a by the radiologist but then it was corrected to 'definiately' a T3a. Now the rating in January was given a T2b/T3a. It is clear that it is difficult to read accurately these tests - that's just the nature of the beast! I seem to be on the borderline between a serious and less serious cancer?
2. PSA climbing.
I have already covered that the PSA is a poor indicator; even the doctor, Richard J. Albin, who created the PSA test says: "PSA testing can’t detect prostate cancer and, more important, it can’t distinguish between the two types of prostate cancer — the one that will kill you and the one that won’t (i)."
So what causes PSA to increase? Basically prostate cancer, benign prostate enlargement (BPH), and prostate inflammation (ii). Some of us have one or two or three of those and it is worth noting that inflammation is an environment that has been shown to encourage tumour growth. Prostate cancer, usually leads to the PSA going up and doesn’t go down unless there is some form of treatment. Apparently BPH is the same, but the increase may not be so steep. Lastly inflammation causes the PSA to go up with a flareup and down as the inflammation lessens.
Dr Daniel George, Professor of Medicine and Professor in Surgery at Duke University (iii), notes that: “there is a strong correlation between a shorter PSA doubling time—a shorter time to bone metastasis—and shorter overall survival...If doubling time is a year or longer, these are slow-growing cancers.”
In terms of my own PSA there are indications of increases but the PSA measure has fluctuated. Is this cancer or inflammation? There is also a link between inflammation and cell death; does that include cancer cells (iv)? I hope the next PSA will give a clearer picture as to whether my PSA is rising or not.
In terms of my own PSA there are indications of increases but the PSA measure has fluctuated. Is this cancer or inflammation? There is also a link between inflammation and cell death; does that include cancer cells (iv)? I hope the next PSA will give a clearer picture as to whether my PSA is rising or not.
3. Gleason questions
I talked about biopsies and Gleason scoring in a previous blog. Elsewhere I note that many, including my doctors, consider a Gleason score of 7 as ‘aggressive’ and ‘invasive’. However the more I learn, the more there are questions. Gleason 6 for many years was treated with prostatectomy or radiation and hormones. Now Active Surveillance is more usually the order of the day and many of the ‘cancers' don’t develop further. In fact there are some doctors now, who argue that it doesn’t really behave like a cancer and could just be part of the ageing process.
Dr Bert Forstmann, while in a minority amongst doctors, writes that: "Only the 15 percent or so of high-grade/high-risk prostate cancers with significant amounts of pattern (grade) 4 and or 5 disease in their Gleason score require detection and treatment as only these types of prostate cancers are potentially deadly.” He then suggests that the "intermediate-risk Gleason 7 category actually includes two very differently behaving prostate cancers; the 3+4=7 and, the 4+3=7. Importantly however, whereas the 3+4 is a low-risk cancer and tends to behave like the bogus G6 especially when it has 10 percent or less of pattern 4 disease — although the exact amount of pattern 4 to be significant is yet to be determined, the 4+3 behaves more like the high-risk Gleason 4+4 and, should be considered for treatment” (v).
So could my Gleason 3+4 be similar to a Gleason 6 and be better considered for Active Surveillance? Or should we be concerned that this is an ‘invasive’ cancer?
Update 4/05/19: Just seen interesting video re Active Surveillance and Gleason scores - see here and another here outlining some of the risks.
Update 4/05/19: Just seen interesting video re Active Surveillance and Gleason scores - see here and another here outlining some of the risks.

Metastasis is what we all want to avoid! I totally get NHS doctors wanting to treat me early to avoid the cancer spreading as prognosis when it spreads is considerably poorer. Indeed doctors say that there is no systemic treatments that can cure metastatic prostate cancer (see here only if you really want to read about horrors of metastasis).
My limited understanding is that high-risk prostate cancer cells basically can’t thrive outside the prostatic environment, but at some point they undergo a genetic transition called epithelial-to-mesenchymal transition (EMT), after which they can freely move throughout the body in the lymph, blood or wherever and accumulate in distant locations. I think 80% of metastasis in prostate cancers go first to the bones; hence when diagnosed with prostate cancer many doctors call for a bone scan. My scan was clear.
Sometimes those microscopic metastases can circulate for a long time before planting themselves somewhere new. Another common place is for them to accumulate in the lymph nodes. I found this video useful in looking at the lymph system differently from many medical doctors; arguing that we should detoxify and exercise to clean out the lymph system rather than perhaps cutting the lymphs out. See Robert Morse ND: https://youtu.be/ScxGrOB1z80
Once metastasis have appeared, there are countless micromets that you can't see in organs, the blood, the lymph and bones. Once some of the mets are large enough to be detected, there are hundreds of thousands more that are too small to be detected by any current technology. I remember reading but can’t find the quote that treatment of metastases has been compared to weeding a garden; you basically keep pulling at the dandelions until there are no more. The person quoting this said that is wrong and a better metaphor would be like plucking mushrooms from under a tree. The fungus mycelium is everywhere, and plucking at the mushrooms doesn't stop it at all. So is it right to hit what you can’t see with, for example, radiation?
The picture is confusing. Metastasis start very slowly. We also know that eliminating the largest mets reduces PSA; this means that after treatment, we can't use PSA progress to monitor effectiveness? What does hitting a met site mean to all those other circulating mets? Yet I totally understand wishes to hit the mets to feel more in control! I’m also aware that there are benefits to hitting weight-bearing bones, which the cancer will weaken over time to prevent fractures, spinal compression, and pain.
So is there a way to see if cancers are about to metastases? A PET scan might give some indications but are not available on NHS for many of us; it also costs close to £2,000. I’ve also come across a number of tests in the alternative and complimentary world, like RGCC or Greek test but again that is close to £2,000.
Two tests that I have done, do give some reassurances that my cancer is not metastasising:
Two tests that I have done, do give some reassurances that my cancer is not metastasising:
(a) High levels of LDL and Triglyceride. Chris Woollams of CancerActive writes: "I have long noted that where prostate cancer patients send me their blood results (PSA, estradiol, oestrone, testosterone, DHT, triglyceride and cholesterol levels), as soon as the triglyceride and cholesterol levels climb, the DHT is not far behind and the cancer is coming back with a vengeance. Research supports this with a big US study showing people with higher levels of blood fat have more metastases and lowered survival times”. In January a test with my GP showed that my triglycerides were the lower end of the normal range and cholesterol has come down since being on my nutrition programme. This hopefully indicates no metastasis.
(b) Nagalase. Nagalase, full name N-acetyl-Galactosaminidase, is an enzyme in the body that helps break down sugar. A company in Stroud coordinates tests for nagalase levels in the body which are considered to help monitoring the effect of therapy in cancer and certain viral infections, including HIV infection (vi). When levels are normal, then that indicates health and the chances of developing cancer are relatively low. However, if higher that means increased tumour cell activity in your body. This is considered a harbinger for cancer. Nagalase levels can also increase in other diseases like viral infections, but this increase has mostly been described for cancer.
The GcMAFplus website writes: “...the amount of nagalase activity in the body corresponds directly to the number of cancer cells in the body as well as tumour size and amount of cancer within the body. It has been demonstrated that by measuring levels of nagalase in the bloodstream it is possible to detect the presence of cancerous lesions well below levels achievable by any other diagnostic means...In summary – Nagalase is an amazingly sensitive marker for each and every type of cancer and allows for the much earlier detection of cancerous lesions than any other known method. It causes immunodeficiency by blocking the development of macrophage activating factor and consecutive nagalase testing is a reliable indicator for tracking the effectiveness of therapeutic regimens for all cancers and certain viral infections (vii).”
My nagalase test result came back mostly normal although one marker was below normal. That has led to an interesting look at why that might be. A further test looking at Genomic DNA from leucocytes found p-dichlorobenzene. This is a pesticide linked to cancer, specifically prostate cancer. Is this a cause or part cause of my cancer? I'm not so sure but certainbly could be a factor? That is yet another blog! Anyhow my nagalase test is another indication of no metastasis. Update 17.05.19: Interesting report looking at why Nagalase test may not be that useful: https://selfhacked.com/blog/nagalase/
5. Current protocol
Well I’ll save the outline of this for another blog in this series, but I want to give the protocol a longer time to further impact on the cancer. As noted previously I had transurethral hyperthermia in Germany followed by six months of hormones that finished last summer. Since last Christmas I am on a new protocol which includes diet and a range of supplements; these have been recommended following a series of blood tests to enhance my immune system and also hopefully impact on the cancer. Update 5/04/19: see protocol here.
Well I’ll save the outline of this for another blog in this series, but I want to give the protocol a longer time to further impact on the cancer. As noted previously I had transurethral hyperthermia in Germany followed by six months of hormones that finished last summer. Since last Christmas I am on a new protocol which includes diet and a range of supplements; these have been recommended following a series of blood tests to enhance my immune system and also hopefully impact on the cancer. Update 5/04/19: see protocol here.
6. NHS Treatment
I want to cover some of my first thoughts regarding the hormone and radiation treatment being offered to me by the NHS. They are big serious treatments and not at all straightforward - and of course don't necessarilly get at teh cause of cancer. So concerns about them also lead to me wanting to see if the protocol I am undertaking will further reduce my tumour. I’ll save these for the next two blogs. Update 4/04/19: see more re hormones here and more re radiotherapy here.
I want to cover some of my first thoughts regarding the hormone and radiation treatment being offered to me by the NHS. They are big serious treatments and not at all straightforward - and of course don't necessarilly get at teh cause of cancer. So concerns about them also lead to me wanting to see if the protocol I am undertaking will further reduce my tumour. I’ll save these for the next two blogs. Update 4/04/19: see more re hormones here and more re radiotherapy here.
Lastly I have been faced with a number of family challenges with the death of my father and my partners father and my mum having a very serious operation. All this and a number of other challenges hasn’t left me with much headspace to plan and also left me reluctant to start treatments that cause so much fatigue and impact on the body.
(i) https://healthbeatblog.com/2010/03/the-doctor-who-invented-psa-test-calls-it-a-profitdriven-public-health-disaster-why-this-is-good-new/
(ii) See more re inflammation: https://www.pcf.org/c/infection-and-prostate-cancer/?fbclid=IwAR2eLHmRaf378Nklc2l1I0C5x5SchmBDEDMuXr1wh63nmHVrwpnVtbyzYX4
(iii) https://www.prostatepedia.net/blogs/prostatepedia/dr-daniel-george-on-psa-recurrence?goal=0_bc8795358a-d7cb05f7bc-199204941&mc_cid=d7cb05f7bc&mc_eid=e7e7fa69da
(iv) https://mmrjournal.biomedcentral.com/track/pdf/10.1186/s40779-015-0039-0
(v) https://medium.com/@bvorstman/is-psa-testing-for-prostate-cancer-bad-health-advice-7199618e56c5?fbclid=IwAR1vufT01HSsN-ShZR5KX-d7cCnVw1KkhgRqvpI4UoMtclTXav7vNGwzz9E
(vi) https://www.invivoclinical.co.uk/products---services/Lab-Diagnostics/Nagalase-Activity
(vii) https://www.gcmafplus.com/about/articles/what-nagalase-how-does-it-affect-cancer
See small study with patients who have prostate cancer: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2510818/



{kind=link}
No comments:
Post a Comment